Clinical Whitepaper
Author: Christos Chapeshis
Date: April 26, 2026
Abstract
Background: Pressure injuries (PIs) are still a critical global healthcare burden despite strong international guidelines. Prevention strategies have traditionally relied on manual repositioning and passive support surfaces; however, real-world adherence remains inconsistent.
Objective: To critically evaluate contemporary pressure injury prevention protocols, focusing on repositioning strategies and support surfaces, and to examine the emerging role of intelligent automated systems, particularly the multiTURN® 6 multifunction automatic lateral turning mattress system.
Methods: Narrative synthesis of high-level evidence, including international guidelines (NPIAP/EPUAP/PPPIA), systematic reviews, and key biomechanical studies. Supplemented by analysis of uploaded guideline documents and comparative effectiveness reports.
Results: Evidence confirms that both magnitude and duration of pressure are central to PI pathophysiology, necessitating combined strategies of pressure redistribution and frequent repositioning. However, manual protocols show considerable variability and limited adherence. Emerging automated systems offer continuous repositioning, improved biomechanical consistency, and the potential to reduce PI incidence.
Conclusion: Intelligent support surfaces such as multiTURN® 6 constitute a paradigm shift from intermittent, labor-dependent care towards continuous, protocol-driven prevention. Further high-quality clinical trials are required, but mechanistic and guideline alignment strongly support their inclusion into modern clinical practice.
Keywords
Pressure injury prevention, pressure ulcer advanced care, repositioning, support surfaces, automated lateral turning, multifunction lateral turning mattress system, MLTM, ABeWER, multiTURN® 6, biomechanical loading, microclimate, clinical innovation, nurses.
Introduction
Pressure injuries are localized damage to the skin and underlying soft tissues, commonly occurring over bony prominences due to sustained mechanical loading. Despite decades of research and the availability of comprehensive clinical practice guidelines, incidence rates remain clinically significant across acute and long-term care settings.
The International Clinical Practice Guideline (2019, updated 2026) stresses a multifactorial prevention strategy that incorporates risk assessment, repositioning, and advanced support surfaces. Nevertheless, translating these recommendations into consistent bedside practice remains suboptimal.
This article analyzes the limitations of traditional prevention strategies and evaluates the role of sophisticated automated systems in addressing these gaps.
Methods
A structured narrative review methodology was applied:
- Primary sources:
- NPIAP/EPUAP/PPPIA Clinical Practice Guidelines (2019, 2026 updates)
- AHRQ Comparative Effectiveness Review on pressure ulcer prevention
- Supplementary sources:
- Biomechanical and clinical reviews on pressure redistribution
- Cochrane systematic reviews and peer-reviewed literature
Evidence synthesis prioritized guideline-level and systematic review data in accordance with accepted evidence hierarchies.
Pathophysiology and Biomechanics of Pressure Injury Formation
Pressure injury development is essentially governed by tissue-loading mechanics, in which both the magnitude and duration of pressure determine cellular damage thresholds.
As highlighted by Sprigle and Sonenblum (2011), pressure injury formation cannot occur without mechanical loading, and tissue tolerance is inversely related to the duration of exposure. This pressure–time relationship underscores the necessity of interventions targeting both variables simultaneously.
Key Mechanisms
- Sustained Pressure: Leads to capillary occlusion, ischemia, and eventual tissue necrosis
- Shear Forces: Distort deep tissues, amplifying damage beyond superficial layers
- Microclimate: Elevated temperature and moisture impair skin resilience
These mechanisms jointly justify the need for dynamic, rather than static, prevention strategies.
Current Standard of Care
Repositioning Protocols
Repositioning continues as a cornerstone of prevention. Guidelines recommend individualized turning schedules, typically every 2–3 hours, adjusted based on patient-specific risk factors.
However, systematic reviews indicate limited high-certainty evidence defining optimal repositioning frequency (Shi et al., 2021). Moreover, adherence is inconsistent in clinical practice.
Support Surfaces
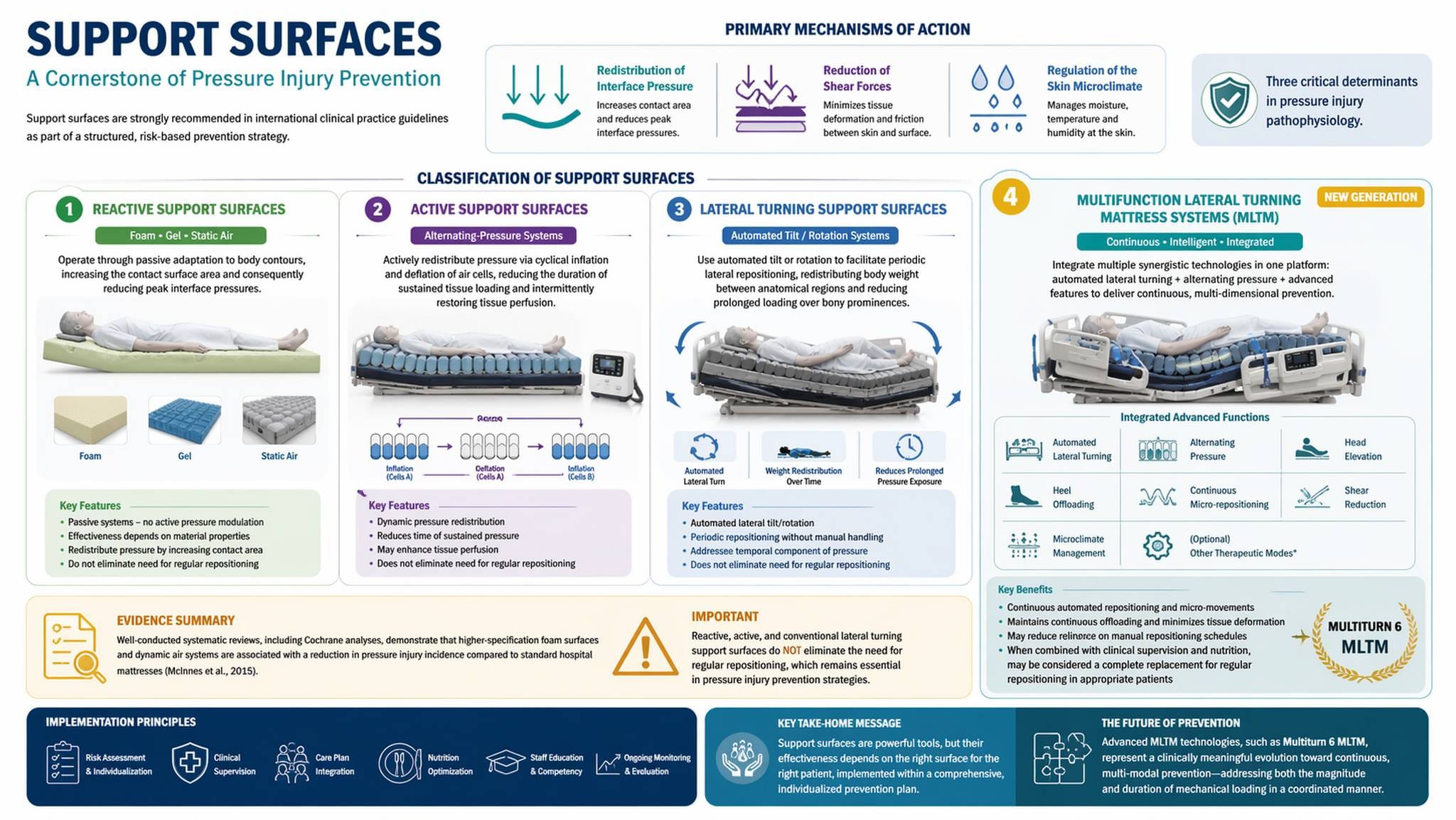
Support surfaces are a mainstay of pressure injury prevention and are strongly recommended in international clinical practice guidelines as part of a structured, risk-based prevention strategy. Their primary mechanisms of action include redistribution of interface pressure, reduction of shear forces, and regulation of the skin microclimate—three critical determinants in pressure injury pathophysiology.
Image 1. Classification of support surfaces and their role in pressure injury prevention.
Support surfaces may be systematically classified into the following categories:
Reactive support surfaces
These include foam, gel, and static air systems. They operate through passive adaptation to body contours, increasing the contact surface area and consequently reducing peak interface pressures. Their effectiveness depends on material properties and does not require active modulation of pressure over time.
Active support surfaces
This category includes dynamic systems, such as alternating-pressure mattresses. These devices actively redistribute pressure via cyclical inflation and deflation of air cells, therewith reducing the duration of sustained tissue loading and intermittently restoring tissue perfusion.
Lateral turning support surfaces
These systems include automated tilt or rotation mechanisms to facilitate periodic lateral repositioning. Through redistributing body weight between anatomical regions, they reduce prolonged loading over bony prominences and partially address the temporal component of pressure exposure.
Evidence derived from well-conducted systematic reviews, including Cochrane analyses, demonstrates that higher-specification foam surfaces and dynamic air systems are associated with a reduction in pressure injury incidence compared to standard hospital mattresses (McInnes et al., 2015). However, in accordance with international guidelines, support surfaces within the reactive, active, and conventional lateral turning categories do not eliminate the need for regular repositioning, which is still an essential part of prevention strategies.
Multifunction Lateral Turning Mattress Systems (MLTM)
This advanced class of support surfaces integrates multiple synergistic technologies within a single platform. These systems combine automated lateral turning with alternating pressure functionality, along with additional features such as head elevation, heel offloading, continuous micro-repositioning, shear reduction, and microclimate control. From a biomechanical perspective, MLTMs represent a transition from intermittent to continuous, multi-dimensional pressure injury prevention, tackling both the magnitude and duration of mechanical loading in a coordinated manner.
Multifunction lateral turning mattress systems (MLTM) deliver continuous automated repositioning and micro-movements, introducing a clinically relevant evolution. That system may reduce reliance on manual repositioning schedules by maintaining continuous offloading and minimizing cumulative tissue deformation. Current guideline frameworks still emphasize that such technologies should be implemented within a supervised, individualized care plan. New high-quality comparative clinical data show the high effectiveness of the advanced multiTURN® 6 MLTM, which demonstrates strong biomechanical and theoretical advantages and can be considered a complete replacement when combined with other prevention strategies, such as clinical supervision and nutrition.
The Implementation Gap
Despite evidence-based recommendations, pressure injuries continue due to systemic limitations.
Workforce Constraints
Manual repositioning is labor-intensive and dependent on staffing ratios. AHRQ data highlight variability in adherence due to workload and care complexity, an issue further explored in the critical role of comprehensive prevention strategies.
Intermittent vs Continuous Care
Traditional protocols operate intermittently, whereas tissue loading is continuous. This mismatch allows cumulative tissue damage between repositioning intervals.
Biomechanical Inconsistency
Manual repositioning causes variability in:
- Offloading angles
- Shear forces during handling
- Repositioning precision
Technological Evolution: Automated Lateral Turning Systems
Automated systems signify a shift toward continuous, controlled repositioning.
Conceptual Advantages
- Elimination of prolonged static loading
- Standardization of repositioning protocols
- Reduction in caregiver-dependent variability
These systems align directly with biomechanical principles identified in the pathophysiology of pressure injuries.
multiTURN® 6: ABeWER’s Advanced Support Surface System
System Definition
multiTURN® 6 is the first multifunction automatic lateral turning mattress system (MLTM) worldwide, developed by ABeWER’s research and development department.
It integrates more than six main functionalities:
- Automated lateral turning
- Continuous micro-repositioning
- Pressure redistribution
- Shear force minimization
- Microclimate regulation
- Programmable positioning protocols
Biomechanical Superiority
From a biomechanical standpoint, multiTURN® 6 addresses both:
- Pressure magnitude → via redistribution
- Pressure duration → via continuous repositioning
This dual-target approach aligns precisely with the mechanistic model described in foundational research.
Conformity with International Guidelines
| Guideline Requirement | multiTURN® 6 Capability |
|---|---|
| Individualized repositioning | Programmable protocols |
| Frequent repositioning | Automated continuous turning |
| Micro-movements | Integrated micro-shifts |
| Shear reduction | Controlled motion mechanics |
| Pressure redistribution | Advanced support surface |
These features operationalize guideline recommendations into automated clinical execution.
Clinical Impact
While large-scale RCTs are still emerging, the system theoretically:
- Enhances adherence to repositioning protocols
- Reduces human error
- Improves consistency of care delivery
- Minimizes caregiver workload
Such benefits directly address the implementation gaps identified in current practice.
Clinical Implications
For Acute Care Settings
- Improved prevention of hospital-acquired pressure injuries (HAPIs)
- Standardization across high-acuity units
For Long-Term Care
- Reduced caregiver burden
- Elevated patient comfort and safety
For Limb Preservation
Particularly relevant in lower-limb pathology, where pressure injuries contribute to:
- Infection risk
- Tissue loss
- Amputation
Combined with stage-specific wound dressing selection, advanced support surfaces address both the mechanical and microenvironmental drivers of tissue damage.
Limitations
- Limited high-quality comparative trials between automated systems and standard care
- Economic analyses remain incomplete
- Inclusion into diverse health care systems requires further study
Additionally, while biomechanical rationale is strong, clinical outcome validation is still evolving.
Future Directions
Future research priorities include:
- Randomized controlled trials evaluating automated systems
- Integration with sensor-based pressure monitoring
- Cost-effectiveness analyses
- Application in high-risk populations (e.g., ICU, diabetic foot patients)
Conclusion
Pressure injury prevention is constrained not by lack of knowledge, but by restrictions in execution.
Traditional strategies—manual repositioning and passive support surfaces—are inherently:
- Intermittent
- Labor-dependent
- Biomechanically inconsistent
multiTURN® 6 represents a clinically rational evolution, transforming prevention into a:
- Continuous
- Standardized
- Technology-enabled process
Aligned with international guidelines and grounded in biomechanical principles, such systems may transform the future standard of care.
References
Berlowitz, D. et al. (2011). Preventing pressure ulcers in hospitals. Agency for Healthcare Research and Quality.
Chou, R. et al. (2013) Pressure Ulcer Risk Assessment and Prevention: Comparative Effectiveness. AHRQ.
European Pressure Ulcer Advisory Panel, National Pressure Injury Advisory Panel, and Pan Pacific Pressure Injury Alliance (2019). Prevention and Treatment of Pressure Ulcers/Injuries: Clinical Practice Guideline.
European Pressure Ulcer Advisory Panel, National Pressure Injury Advisory Panel, and Pan Pacific Pressure Injury Alliance (2026). Prevention and Treatment of Pressure Ulcers/Injuries: Quick Reference Guide.
McInnes, E. et al. (2015) ‘Support surfaces for pressure ulcer prevention’, Cochrane Database of Systematic Reviews, CD001735.
Padula, W.V. and Delarmente, B.A. (2019) ‘The national cost of hospital-acquired pressure injuries in the United States’, International Wound Journal, 16(3), pp. 634–640.
Shi, C. et al. (2021) ‘Repositioning for preventing pressure ulcers’, Cochrane Database of Systematic Reviews, CD009958.
Sprigle, S. and Sonenblum, S. (2011) ‘Assessing evidence supporting redistribution of pressure for pressure ulcer prevention’, Journal of Rehabilitation Research & Development, 48(3), pp. 203–214.
Brienza, D. et al. (2022) ‘The vision and scope of the prophylactic dressing standard initiative’, International Wound Journal.